
Ban Xia Xie Xin Tang

In the Summer of 2023, whilst completing my DAcHm program, I completed a mandatory research class. Many chose to do a meta-analysis of acupuncture points and protocols. I feel more pulled to work with herbs, thus leading me on a dive to find RCTs (randomized control trials) about traditional Chinese medicine botanical formulas. It was my first introduction to learning how to find what I was looking for in this realm of knowledge. The curiosity of the plants, or rather ethnobotany, has always fascinated me. Whilst it was a challenge to find enough papers to support a theory of using an herbal formula to help a diagnosed bio-medical disease, and also showing the pattern it treats in the Eastern medical diagnosis, I delved into a world that truly captivated me. I finally settled on a formula and found through a meta-analysis paper that it is indeed often used alongside biomedical treatments for chronic atrophic gastritis, a condition that affects about twenty-five percent of the world population.
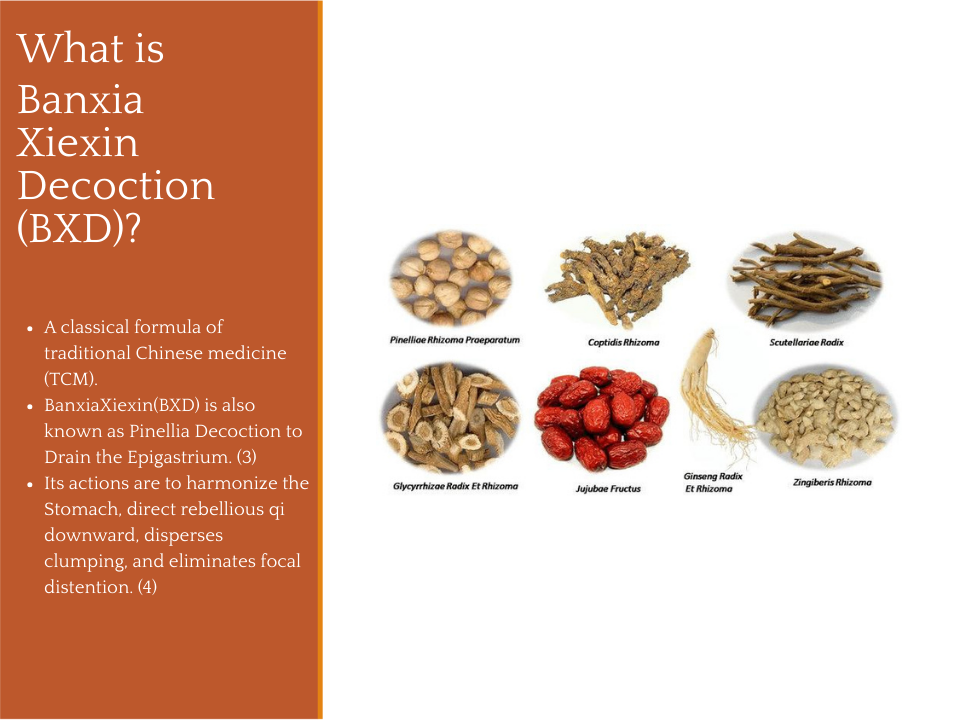
The formula known as Banxia Xiexin (BXD or BXXXD) is also known as Pinella Decoction to Drain the Epigastrium. (Scheid, 2015, p. 127) 5 The formula consists of 7 herbs: zhi ban xia/Pinelliae Rhizoma, gan jiang/Zingiberis Rhizoma, huang qin/Scutellariae Radix, huang lian/Coptidis Rhizoma, ren shen/Ginseng Radix, da zao/Jujubae Fructus, and da zao/Glycyrrhizae Radix praeparata.
I sought out randomized control trials that focused on the use of the traditional Chinese medicine formula known as Ban Xia Xie Xin Tang. Through the dissection of the meta-analysis study, I saw the benefits of the herbal formula Banxia Xiexin and understood that further study would support the efforts already made by studying and including more long-term studies because of the high recurrence rate of gastritis.
Ban Xia Xie Xin Tang is usually used for patients with a pattern known as both a cold and heat complex. According to Chinese Herbal Medicine: Formulas & Strategies (Portable 2nd ed.) by Scheid, V., Bensky, D., Ellis, A., & Barolet, R., Eastland Press, patients usually present with epigastric focal distention, fullness, and tightness with very slight or no pain, dry heaves or frank vomiting (also known as hematemesis or vomiting of blood), borborygmus (rumbling or gurgling noises in the intestines caused by gas and fluids) with diarrhea, and a reduced appetite. Their tongue coating may present with a red tip, whilst their pulse may feel wiry and rapid (If you don’t understand traditional Chinese medicine pulse diagnosis, you can read about it here).
Ban Xia Xie Xin Tang is commonly used for presents as improper purging of an exterior or half-exterior, half-interior condition in a patient with underlying Spleen and Stomach deficiency. Please understand that TCM (traditional Chinese medicine) diagnosis is not the same as a biomedical diagnosis. Spleen in TCM is related to the digestive system, whereas in bio-medicine it is related to the immune system. That said, this condition is not always considered an improper purging. It can also arise whenever the ascending and descending-directing functions of the Spleen and Stomach are disturbed by the presence of dampness or phlegm constraining the middle burner yang.
From a biomedical perspective and diganosis this is quite often gastritis, a condition the inflammation, irritation, or erosion of the protective lining of the stomach (mucosa). Gastritis can be caused by long-term NSAID use (aspirin, ibuprofen), alcohol misuse, smoking, severe stress, and autoimmune diseases. However, the most common cause is infection with Helicobacter pylori bacteria (H. pylori). Gastritis can also lead to chronic atrophic gastritis cases, which is a long-term condition characterized by inflammation, thinning (atrophy), and loss of specialized cells in the stomach lining, often leading to intestinal metaplasia (also known as IM, which is a precancerous condition where the lining of the stomach or esophagus changes, developing cells similar to the small intestine).
The publication Population-Based Helicobacter pylori Screen-and-Treat Strategies for Gastric Cancer Prevention: Guidance on Implementation shares that gastric cancer is the fifth most commonly diagnosed cancer and the fifth leading cause of cancer death worldwide, with an age-standardized incidence rate of 9.2 per 100,000 person-years and an age-standardized mortality rate of 6.1 per 100,000 person-years in 2022 [8]. In absolute numbers, an estimated 969,000 new cases of gastric cancer (4.8% of all cancer cases) were diagnosed, and 660,000 deaths from gastric cancer (6.8% of all cancer deaths) occurred in 2022 [1].
A wide variation in gastric cancer incidence and mortality rates is observed across world regions (Fig. 1.1). The regions of eastern Asia (male ASR, 23.0 per 100 000 person-years; female ASR, 9.7 per 100 000 person-years; 521 000 new cases combined) and eastern Europe (male ASR, 16.2; female ASR, 7.7; 66 400 new cases combined) have the highest incidence rates. By World Health Organization (WHO) region, the Western Pacific Region has the highest incidence (ASR, 15.2; 543 757 new cases), followed by the European Region (ASR, 8.4; 161 553 new cases), the Eastern Mediterranean Region (ASR, 6.6; 37 781 new cases), the Region of the Americas (ASR, 6.4; 103 924 new cases), the South-East Asia Region (ASR, 4
With the most common cause of chronic atrophic gastritis being Helicobacter pylori (H. pylori) infection or autoimmune destruction, it is considered a pre-malignant condition that can lead to stomach cancer, requiring regular endoscopic surveillance. Though I must interject, I don’t know if I fully support the idea of completely eradicating h. plylori. There is more research, and we have a long way to go, that is looking at possibly healing the gut microbiome to allow it to be there, but in check. There is a podcast hosted by Judy Cho where she interviews Dr. Neill Stollman, a recognized expert on the gut microbiome, treatment of C. Difficile and Fecal Microbiota Transplant (FMT), diverticular disease, H. pylori infection, acid reflux disease, and eosinophilic esophagitis, on this very subject of balance and not necessarily complete erdatication, and I highly recommend and encourage a listen.
Equally the same with H. pylori, where “the more cytotoxic the strain is, the more active, and, obviously, the more aggressive is the chronic gastritis. The most aggressive forms of chronic gastritis are those that result most likely in advanced stages of atrophic gastritis, i.e., are forms of H. pylori gastritis with the highest likelihood to progress to the end-stage atrophy. The annual risk of progression of chronic gastritis from one step to the next is estimated to be 2–3% on average. It is estimated further that ∼50% of patients with chronic gastritis (and H. pylori infection) will get atrophic gastritis of some grade and extent during their lifetime. In some 5% of the infected people, atrophic gastritis will get to a severe and advanced stage.”Sipponen, P., & Maaroos, H. I. (2015)) 4
The results were statistically significant; BXD showed statistically significant differences in clinical efficacy rate compared to the control group (RR 1.29; 95% CI 1.24, 1.35; P<0.00001). The test for overall effects: Z = 11.41. It showed that the clinical efficacy rate of BXD was better than the control group. (Cao, Y., Zheng, Y., Niu, J., Zhu, C., Yang, D., Rong, F., & Liu, G. (2020))
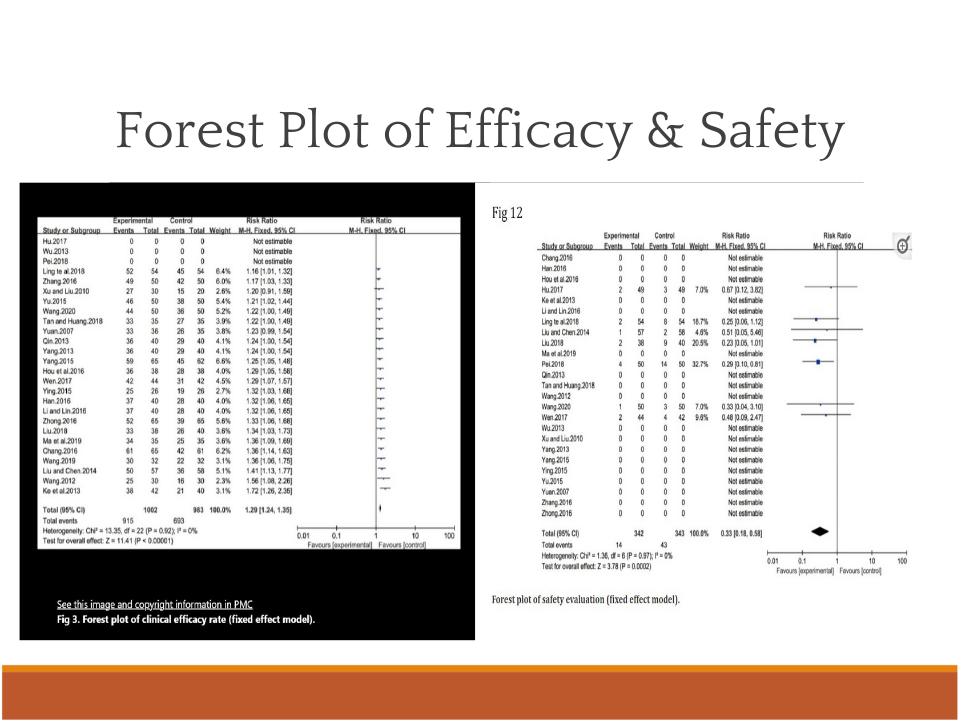
Among the included studies, twenty-three [13,14,17–30,32–38] reported the clinical efficacy rate. Heterogeneity analysis results (P = 0.92, I2 = 0%) showed homogeneity among 23 studies, so a fixed effect model was used for analysis. BXD showed statistically significant differences in clinical efficacy rate compared to the control group (RR 1.29; 95% CI 1.24, 1.35; P<0.00001). The test for overall effects: Z = 11.41. It showed that the clinical efficacy rate of BXD was better than that of the control group.” (Cao, Y., Zheng, Y., Niu, J., Zhu, C., Yang, D., Rong, F., & Liu, G. (2020))
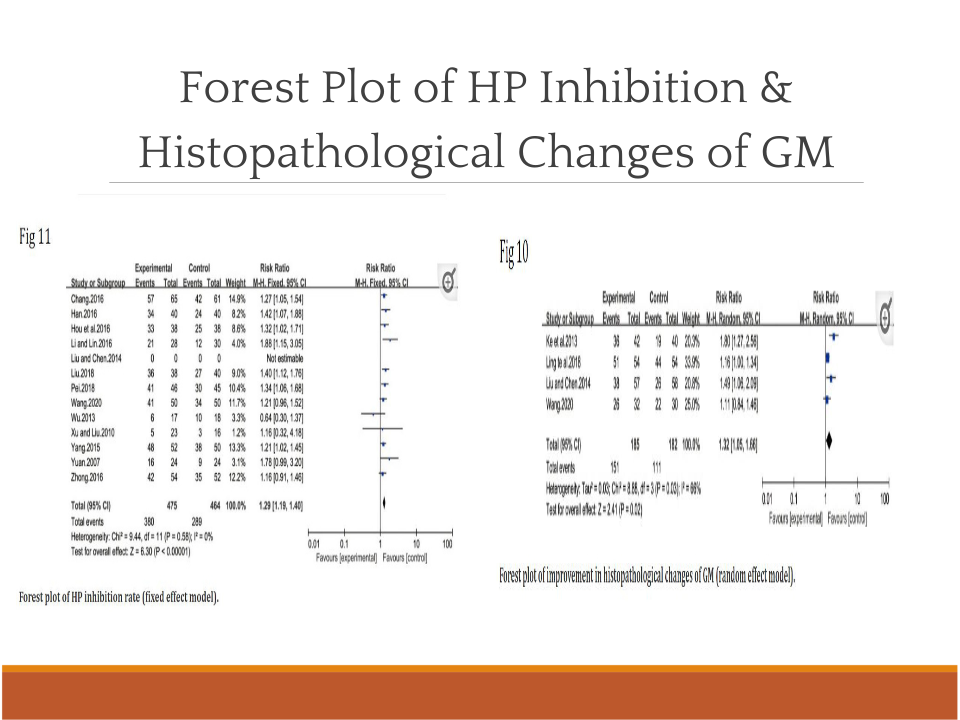
For the HP inhibition rate, “thirteen of all the included studies [15,18–21,23,24,27,31,33–35,37–38] reported the improvement of the HP inhibition rate after treatment. The results of the heterogeneity test were P = 0.58 and I2 = 0%, which showed that the study had homogeneity, so the fixed effect model was adopted for analysis. BXD showed statistically significant differences in HP inhibition rate compared to the control group (MD 1.29; 95% CI 1.19, 1.40; P<0.00001). The test for overall effects: Z = 6.30. The results showed that the HP inhibition rate in CAG patients with BXD was better than that of the control group (Fig 11).” (Cao, Y., Zheng, Y., Niu, J., Zhu, C., Yang, D., Rong, F., & Liu, G. (2020)).
For the histopathological changes, four of all the included studies [13,27,30,38] reported the improvement in histopathological changes of GM after treatment, including glandular atrophy, IM, and dysplasia. The result of the heterogeneity test was I2 = 66%, which showed that the study had heterogeneity, so the random effect model was adopted for analysis. BXD showed statistically significant differences in the improvement of histopathologic changes of GM compared to the control group (MD 1.32; 95% CI 1.05, 1.66; P = 0.02). The test for overall effects: Z = 2.41. The results showed that histopathologic changes of GM in CAG patients with BXD were better than those of the control group (Fig 10).” (Cao, Y., Zheng, Y., Niu, J., Zhu, C., Yang, D., Rong, F., & Liu, G. (2020)).
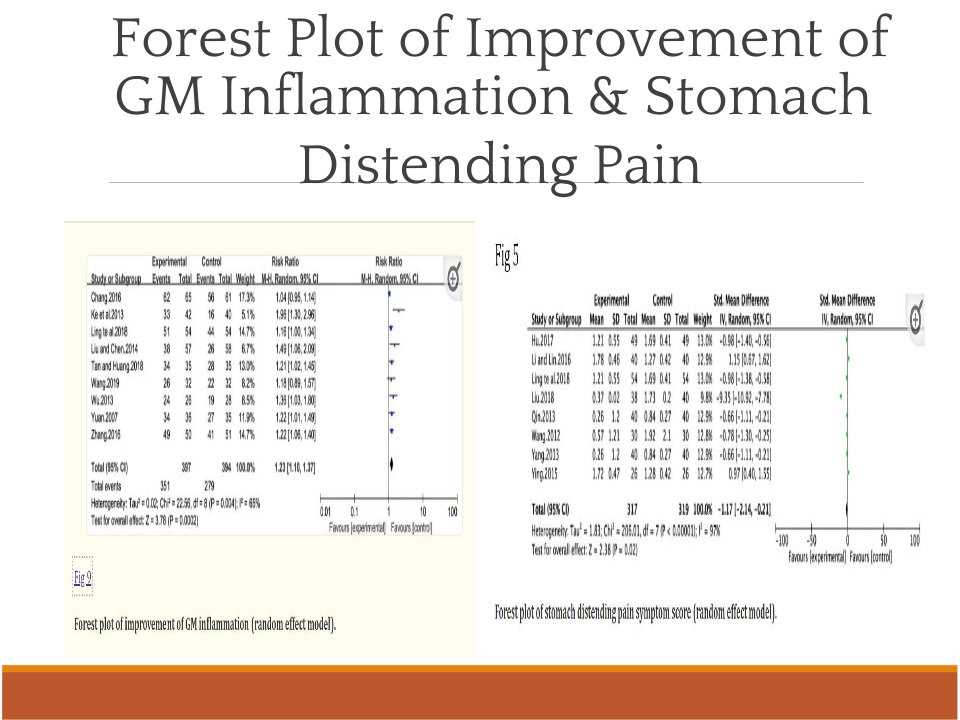
Regarding the stomach distending pain symptom score, “eight of all the included studies [13,16,21,26,28,29,32,35] reported the improvement of the stomach distending pain symptom score. The heterogeneity test results were I2 = 97%, indicating that the study had heterogeneity, so the random effect model was adopted for analysis. BXD showed statistically significant differences in stomach distending pain symptoms compared to the control group (WMD -1.17; 95% CI -2.14, -0.21; P = 0.02). The test for overall effects: Z = 2.38. The results showed that the stomach distending pain symptom in CAG patients with BXD was better than the control group (Fig 5).” (Cao, Y., Zheng, Y., Niu, J., Zhu, C., Yang, D., Rong, F., & Liu, G. (2020))
For the improvement of gastric mucosa inflammation, nine of all the included studies [13,14,22,24,27,30,31,34,37] reported improvement of GM inflammation on CAG patients after BXD treatment. The result of the heterogeneity test was I2 = 65%, indicating that the study had heterogeneity, so the random effect model was adopted for analysis. BXD showed statistically significant differences in improvement of GM inflammation compared to the control group (MD 1.23; 95% CI 1.10, 1.37; P = 0.0002). The test for overall effects: Z = 3.78. The results showed that the improvement of GM inflammation in CAG patients with BXD was better than that of the control group (Fig 9).” (Cao, Y., Zheng, Y., Niu, J., Zhu, C., Yang, D., Rong, F., & Liu, G. (2020)).
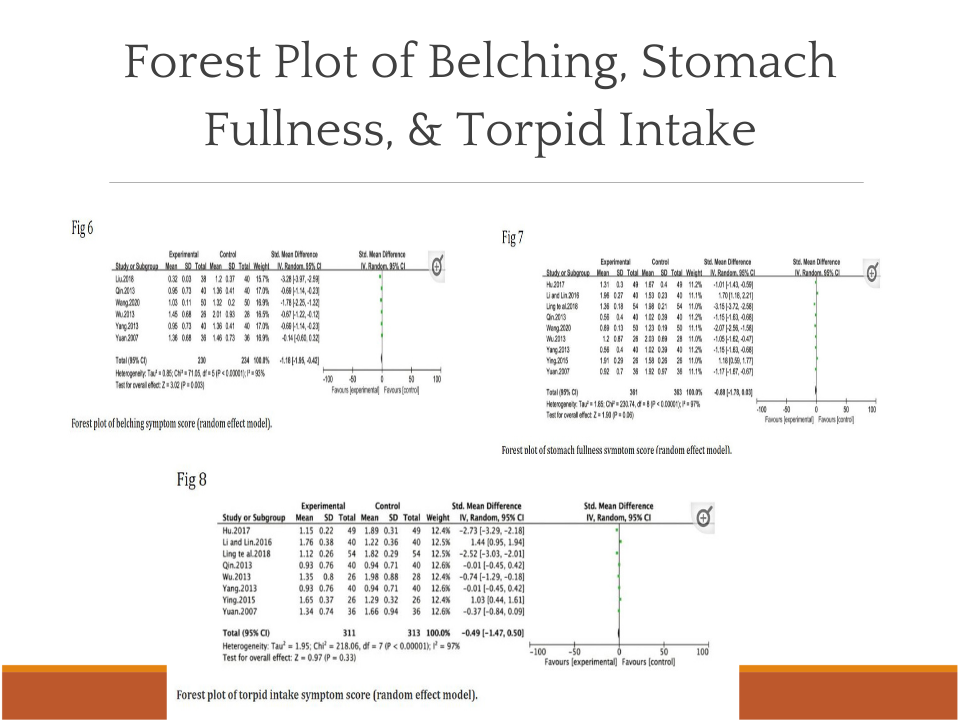
For the belching symptom results, six of all the included studies [28,29,31,34,35,38] reported the improvement of the belching symptom score. The heterogeneity test results were I2 = 93%, indicating that the study had heterogeneity, so the random effect model was adopted for analysis. BXD showed statistically significant differences in belching symptoms compared to the control group (WMD -1.18; 95% CI -1.95, -0.42; P = 0.003). The test for overall effects: Z = 3.02. The results showed that the belching symptom in CAG patients with BXD was better than in the control group (Fig 6). (Cao, Y., Zheng, Y., Niu, J., Zhu, C., Yang, D., Rong, F., & Liu, G. (2020))
Overall, the analysis of symptom results showed that BXD had advantages in improving the symptoms of stomach distending pain and belching, but BXD had no obvious effects on stomach fullness symptoms and torpid intake symptoms.
The meta-analysis concluded that the control trials showed that BXD was more effective and safer for patients with chronic atrophic gastritis than the control group. Future research is necessary to determine the long-term validity of these trials. The sample sizes were small, and the trials were short with little to no follow-up.
It was my goal in reviewing this meta-analysis paper to discover whether or not there was an efficacy for chronic atrophic gastritis using the herbal formula Banxia Xiexin. The curiosity of helping my family and others with chronic atrophic gastritis led me to search for herbal formulas that could assist with the success of the plaguing condition, which is known to lead to gastric cancer. The review led me to many databases, and in this discovery, I learned that this formula was statistically significant in helping to heal conditions related to chronic atrophic gastritis, but still needs long-term research to determine just how consistently effective it could be on this disease.
In the end, I am satisfied with the results that have been done and I hope to be part of future research using this herbal decoction myself, as well as to treat patients and possibly eradicate the disease of chronic atrophic gastritis and precancerous lesions which in turn would hopefully prevent stomach cancer, canceling one of the serious diseases that is the fifth leading causes of cancer mortality worldwide.
The information shared on this website and in associated offerings is provided for educational and informational purposes only. It is not intended to diagnose, treat, cure, or prevent any disease, nor is it a substitute for licensed medical or psychological care.
I am not acting as a medical provider. Always consult a qualified healthcare practitioner before beginning any new wellness or herbal practice, especially if you are pregnant, nursing, taking medications, or managing a medical condition.